Your Brain Has Many Pathways, And TMS Can Now Use Them
May 21, 2026
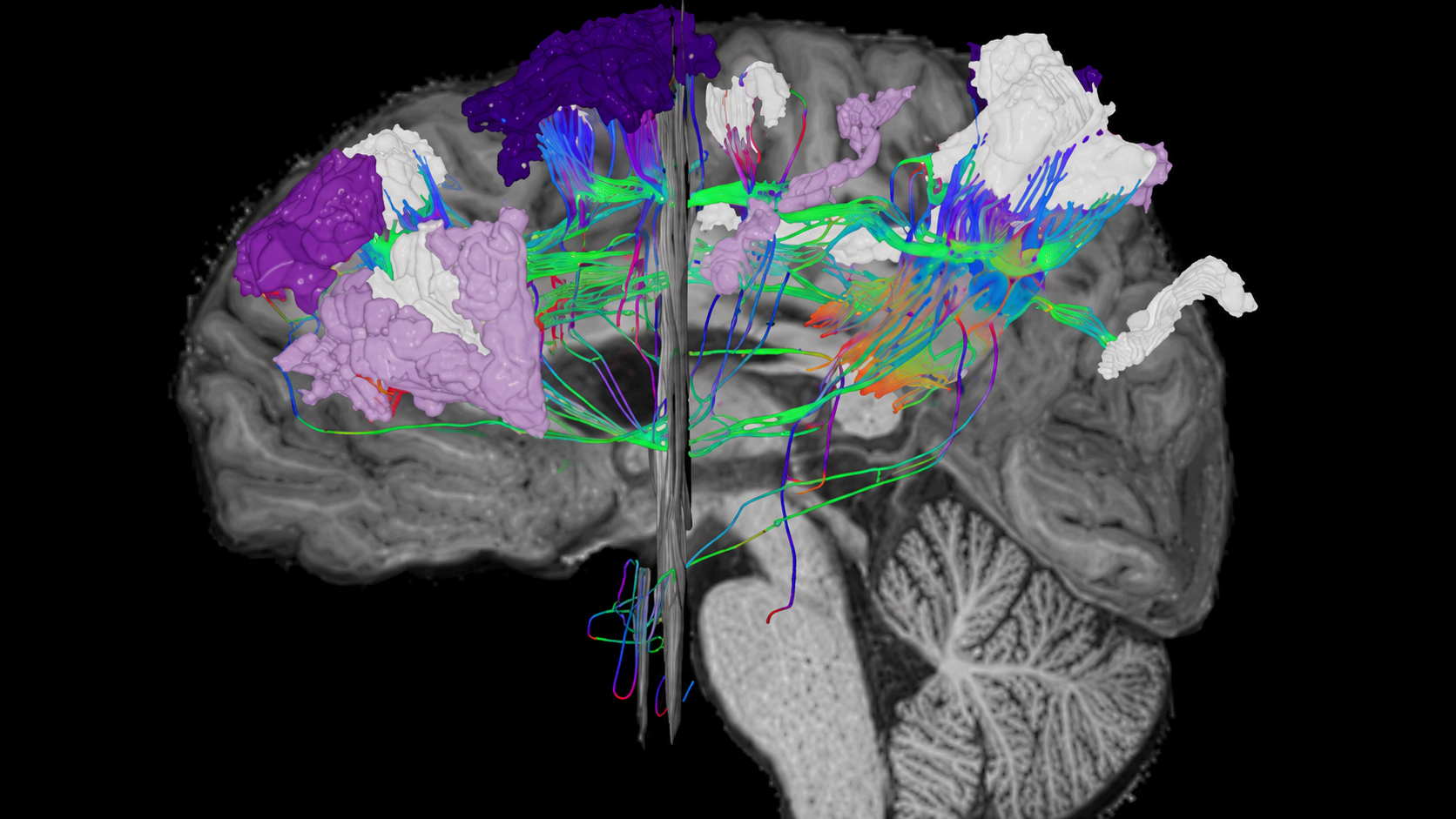
A groundbreaking University of Iowa study shows that personalized fMRI-guided TMS can now reach and modulate the deep hippocampus — the brain’s command center for memory, emotion, and migraine — without surgery or heavy medications.
By mapping each patient’s unique neural pathways, TMS delivers precise stimulation to surface “control points” that influence deep brain structures. Generic approaches barely work, but individualized targeting produces clear, measurable changes.
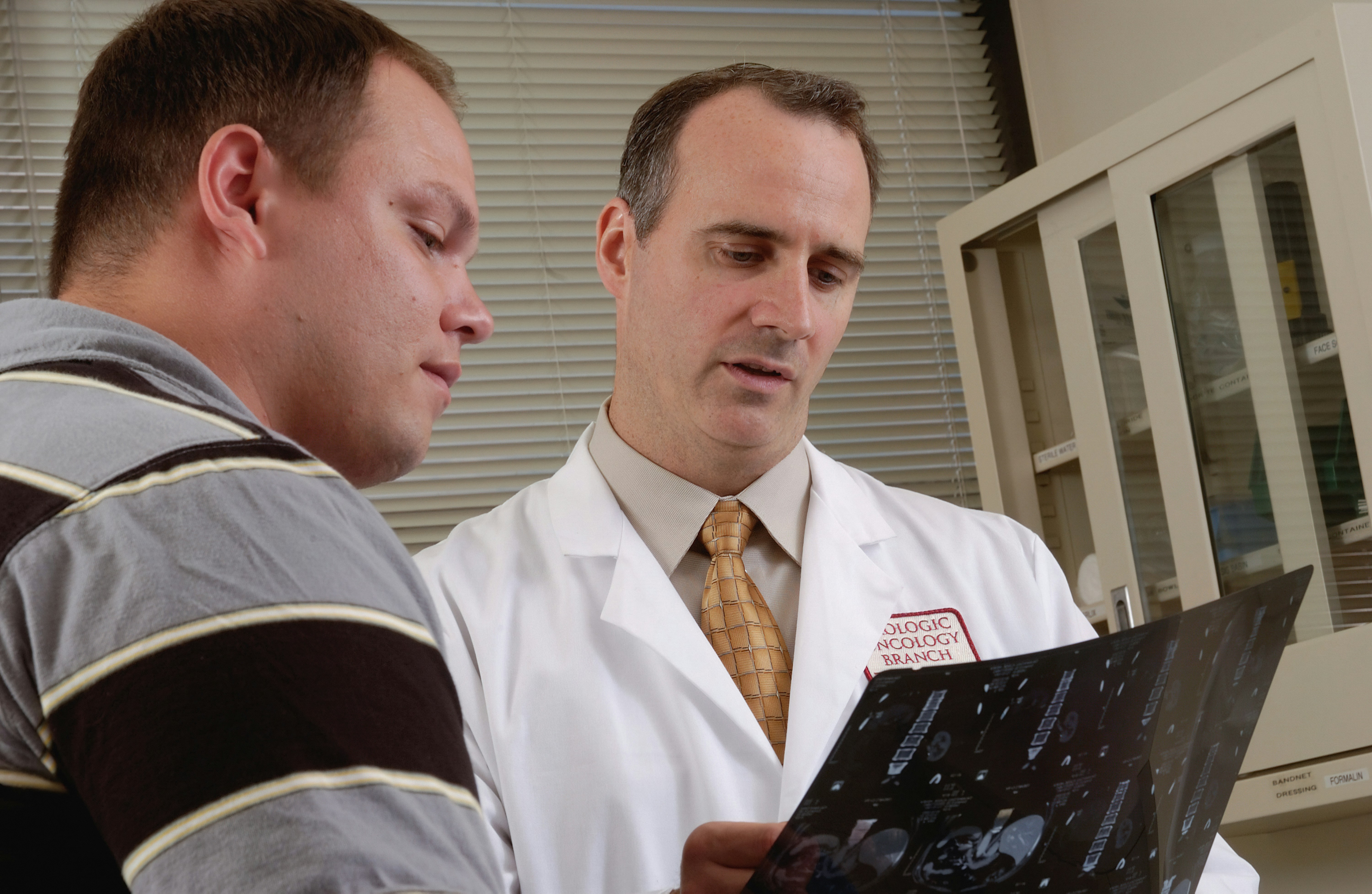
At our headache clinic, we combine TMS and fMRI to offer this advanced, personalized treatment for migraines, depression, PTSD, anxiety, and more.
Read article




.avif)
.jpg)